Resistance is (not) futile.
December 13, 2010 8:36 AM Subscribe
Can somebody give me the current lowdown on antibiotic resistance?
It appears at this point docs are sometimes still doling out the same antibiotics that they were 20 years ago. Although my ENT doesn't have a problem going to something like Levaquin pretty quickly. Is this because they are hoping that the old skool antibiotics will still nuke whatever it is you have that isn't say, antibiotic-resistant MRSA in particular? (So, the increasingly resistant bacterial strains are only of a particular infectious type?) Does the specialty of a doc affect which antibiotic they'll go to first?
I did read this recent Newsweek article which says in part: "The CDC estimates that as much as 50 percent of all antibiotic use is unnecessary. Doctors routinely prescribe antibiotics as a precautionary measure, to ward off infections that have not yet occurred, or to appease patients worried about falling ill while on the road. And for patients who are infected, the approach is hardly more sophisticated. Most diagnostic methods pre-date penicillin, which is to say they are slow, cumbersome, and unreliable. This means doctors often have no way of knowing which bug a patient is infected with, or which drugs that bug might be susceptible to. Rather than waste time and money trying to answer those basic questions, they often prescribe a couple of antibiotics at once and then just cross their fingers. This approach is cheaper, and in the short term it works, but it also contributes to overuse and thus allows resistance to grow and spread."
also: GAH!!! "in 2009 several large chain pharmacies began giving away free generic antibiotics in an effort to lure more customers."
It appears at this point docs are sometimes still doling out the same antibiotics that they were 20 years ago. Although my ENT doesn't have a problem going to something like Levaquin pretty quickly. Is this because they are hoping that the old skool antibiotics will still nuke whatever it is you have that isn't say, antibiotic-resistant MRSA in particular? (So, the increasingly resistant bacterial strains are only of a particular infectious type?) Does the specialty of a doc affect which antibiotic they'll go to first?
I did read this recent Newsweek article which says in part: "The CDC estimates that as much as 50 percent of all antibiotic use is unnecessary. Doctors routinely prescribe antibiotics as a precautionary measure, to ward off infections that have not yet occurred, or to appease patients worried about falling ill while on the road. And for patients who are infected, the approach is hardly more sophisticated. Most diagnostic methods pre-date penicillin, which is to say they are slow, cumbersome, and unreliable. This means doctors often have no way of knowing which bug a patient is infected with, or which drugs that bug might be susceptible to. Rather than waste time and money trying to answer those basic questions, they often prescribe a couple of antibiotics at once and then just cross their fingers. This approach is cheaper, and in the short term it works, but it also contributes to overuse and thus allows resistance to grow and spread."
also: GAH!!! "in 2009 several large chain pharmacies began giving away free generic antibiotics in an effort to lure more customers."
If what you have isn't resistant to a particular antibiotic, then yes, that antibiotic will be effective against the infection.
Antibiotics are frequently also broken down into "broad spectrum" and "narrow spectrum." As the names would suggest, broad spectrum is effective against a wide array of infections, but frequently broad spectrum antibiotics have a low therapeutic index. If you are a doctor seeing a patient with an unknown bacterial infection and you suspect the patient to be terminally ill, you'll probably prescribe a broad spectrum antibiotic first, and then when you form a more specific diagnosis you can switch to narrow spectrum.
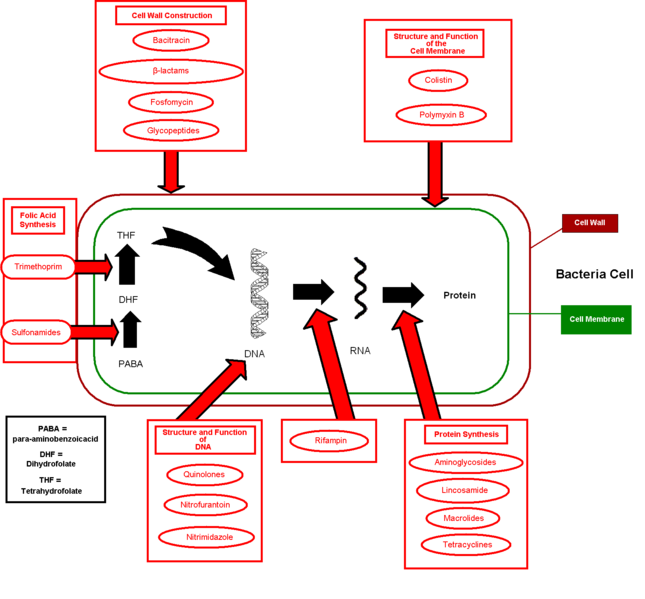
Also, antibiotics work via an array of different mechanisms. Levaquin for instance, is a fluoroquinolone, which is a class of antibiotics that target the DNA gyrase topoisomerase. Other antibiotics may target bacterial ribosomes, which are responsible for protein synthesis. Penicillins are beta-lactams and competitively inhibit binding proteins.
Certain strains of bacteria develop resistance by increasing efflux out of the cell, decreasing uptake into the cell, modifying the antibiotic target site, inactivating the drug through hydrolysis or derivitization, or just metabolically bypassing the process that made the antibiotic effective to begin with. Therefore, if your doctor uses an antibiotic and it doesn't work, what other option is there than to try something else?
Sometimes, if you find that a person has come down with an infection from a resistant strain, you have the alternative of prescribing a drug that targets the infection via a different mechanism. One example is oxazolidinones, which are effective against a wide variety of Gram positive bacteria and are frequently used when dealing with an infection from a β-lactam and/or vancomycin resistant strain.
And yes, doctors prescribe antibiotics as a precautionary measure, especially when someone is immunocompromised. Nosocomial infections are serious and can be deadly.
posted by Demogorgon at 9:07 AM on December 13, 2010 [3 favorites]
Antibiotics are frequently also broken down into "broad spectrum" and "narrow spectrum." As the names would suggest, broad spectrum is effective against a wide array of infections, but frequently broad spectrum antibiotics have a low therapeutic index. If you are a doctor seeing a patient with an unknown bacterial infection and you suspect the patient to be terminally ill, you'll probably prescribe a broad spectrum antibiotic first, and then when you form a more specific diagnosis you can switch to narrow spectrum.
Also, antibiotics work via an array of different mechanisms. Levaquin for instance, is a fluoroquinolone, which is a class of antibiotics that target the DNA gyrase topoisomerase. Other antibiotics may target bacterial ribosomes, which are responsible for protein synthesis. Penicillins are beta-lactams and competitively inhibit binding proteins.
Certain strains of bacteria develop resistance by increasing efflux out of the cell, decreasing uptake into the cell, modifying the antibiotic target site, inactivating the drug through hydrolysis or derivitization, or just metabolically bypassing the process that made the antibiotic effective to begin with. Therefore, if your doctor uses an antibiotic and it doesn't work, what other option is there than to try something else?
Sometimes, if you find that a person has come down with an infection from a resistant strain, you have the alternative of prescribing a drug that targets the infection via a different mechanism. One example is oxazolidinones, which are effective against a wide variety of Gram positive bacteria and are frequently used when dealing with an infection from a β-lactam and/or vancomycin resistant strain.
And yes, doctors prescribe antibiotics as a precautionary measure, especially when someone is immunocompromised. Nosocomial infections are serious and can be deadly.
posted by Demogorgon at 9:07 AM on December 13, 2010 [3 favorites]
As Demogorgon said, there's the matter of broad spectrum verses narrow spectrum targeted drugs. There's also the issue of mechanism of action, which is also what I think Demo was getting at. Many antibiotic resistant strains have mutated such that a previously specifically or generally targeted antibiotic no longer affects the same target site in their structure that the antibiotic would before.
And then, on top of this, you have populations of bacteria that develop multi-drug or single drug tolerances, which while not as problematic as resistances, can be very problematic for an individual case.
Further complicating this, some individuals have either very specific or quite general allergies to different antibiotics, which limits what can be used on their specific infection.
posted by strixus at 9:34 AM on December 13, 2010
{kind=link}
And then, on top of this, you have populations of bacteria that develop multi-drug or single drug tolerances, which while not as problematic as resistances, can be very problematic for an individual case.
Further complicating this, some individuals have either very specific or quite general allergies to different antibiotics, which limits what can be used on their specific infection.
posted by strixus at 9:34 AM on December 13, 2010
also: GAH!!! "in 2009 several large chain pharmacies began giving away free generic antibiotics in an effort to lure more customers."
Well, to be fair on this point, pharmacists don't go throwing antibiotics out into crowds, after all. They do still require a prescription. And in my experience the drugs that are free are generally limited to the older, more "safe" antibiotics (i.e., not Levaquin and the like). So I don't think THIS is contributing all that much to the problem. At least I would hope doctors aren't prescribing more just because their patients ask because they know it's free.
posted by eldiem at 9:43 AM on December 13, 2010
Well, to be fair on this point, pharmacists don't go throwing antibiotics out into crowds, after all. They do still require a prescription. And in my experience the drugs that are free are generally limited to the older, more "safe" antibiotics (i.e., not Levaquin and the like). So I don't think THIS is contributing all that much to the problem. At least I would hope doctors aren't prescribing more just because their patients ask because they know it's free.
posted by eldiem at 9:43 AM on December 13, 2010
Best answer: While the overprescription problem is real, it is dwarfed by the widespread use of antibiotics at factory farms.
If you're looking for someone to blame, start there.
posted by overhauser at 9:46 AM on December 13, 2010 [5 favorites]
If you're looking for someone to blame, start there.
posted by overhauser at 9:46 AM on December 13, 2010 [5 favorites]
Does the specialty of a doc affect which antibiotic they'll go to first?
To the extent that some kinds of bacteria are more common in various specialties, yes. A dermatologist can guess that a minor skin infection or acne is probably caused by one of a handful of bacteria that respond to certain antibiotics, while a GI doc would expect to be dealing with a different subset of bacteria and would therefore prescribe the drugs that are more likely to be effective against those types of bugs.
Doctors routinely prescribe antibiotics as a precautionary measure, to ward off infections that have not yet occurred
This can be remarkably important, such as in surgical patients or the immunocompromised. The infections that are being prevented are not minor little things, they can be deadly. Obviously giving someone a random antibiotic before they travel, "just in case they get something," is not helpful. But prophylactic antibiotics certainly are appropriate in a variety of circumstances.
This means doctors often have no way of knowing which bug a patient is infected with, or which drugs that bug might be susceptible to.
While this may be true for minor infections that are treated in the clinic, almost any infection in the hospital is cultured before antibiotics are started. That means a sample is collected from the infected area (whether urine, stool, nasal secretions, wound fluid, etc.), then grown in the lab. This allows the lab people to identify what kind of bacteria is growing. The sample is also grown on plates with tiny antibiotic buttons to see which kinds of drugs will kill or stop the growth of that particular kind of bacteria. This quote that the "doctors often have no way of knowing" is really misleading, because this test is their way of knowing. The doctor may start a broad-spectrum antibiotic as soon as the sample is collected, in hopes of stopping or slowing the infection while waiting on these results, but once the data is in it may make sense to switch to a more effective antibiotic.
posted by vytae at 9:52 AM on December 13, 2010
To the extent that some kinds of bacteria are more common in various specialties, yes. A dermatologist can guess that a minor skin infection or acne is probably caused by one of a handful of bacteria that respond to certain antibiotics, while a GI doc would expect to be dealing with a different subset of bacteria and would therefore prescribe the drugs that are more likely to be effective against those types of bugs.
Doctors routinely prescribe antibiotics as a precautionary measure, to ward off infections that have not yet occurred
This can be remarkably important, such as in surgical patients or the immunocompromised. The infections that are being prevented are not minor little things, they can be deadly. Obviously giving someone a random antibiotic before they travel, "just in case they get something," is not helpful. But prophylactic antibiotics certainly are appropriate in a variety of circumstances.
This means doctors often have no way of knowing which bug a patient is infected with, or which drugs that bug might be susceptible to.
While this may be true for minor infections that are treated in the clinic, almost any infection in the hospital is cultured before antibiotics are started. That means a sample is collected from the infected area (whether urine, stool, nasal secretions, wound fluid, etc.), then grown in the lab. This allows the lab people to identify what kind of bacteria is growing. The sample is also grown on plates with tiny antibiotic buttons to see which kinds of drugs will kill or stop the growth of that particular kind of bacteria. This quote that the "doctors often have no way of knowing" is really misleading, because this test is their way of knowing. The doctor may start a broad-spectrum antibiotic as soon as the sample is collected, in hopes of stopping or slowing the infection while waiting on these results, but once the data is in it may make sense to switch to a more effective antibiotic.
{kind=link}
posted by vytae at 9:52 AM on December 13, 2010
Response by poster: Thanks for the answers, folks!!
chris - I will check out Superbug, thx.
Demo / vytae - What I still don't get is, shouldn't there be some antibiotics, then, that are completely useless now (or very unlikely to do jack) based on this evidence? If so, why are they still being sold? And the resistance is, or is not, growing across the board for all types of infectious bacteria?
For example: I walked into a clinic yesterday for a presumed sinus infection (I'm pretty darn sure it is, just knowing what they feel like for me), and after talking with the guy and him having examined my grossness, he prescribed amoxicilllin. I remember taking that as a kid, so I'd think the likelihood of it helping now is slim. No?
posted by bitterkitten at 10:09 AM on December 13, 2010
chris - I will check out Superbug, thx.
Demo / vytae - What I still don't get is, shouldn't there be some antibiotics, then, that are completely useless now (or very unlikely to do jack) based on this evidence? If so, why are they still being sold? And the resistance is, or is not, growing across the board for all types of infectious bacteria?
For example: I walked into a clinic yesterday for a presumed sinus infection (I'm pretty darn sure it is, just knowing what they feel like for me), and after talking with the guy and him having examined my grossness, he prescribed amoxicilllin. I remember taking that as a kid, so I'd think the likelihood of it helping now is slim. No?
posted by bitterkitten at 10:09 AM on December 13, 2010
I am by no means an expert here, but my understanding is that if a portion of a bacterial population evolves a resistance to a particular antibiotic, that resistance won't necessarily persist for very many generations after the resistance develops; the drug-resistance phenotype may be an advantage inside a host that is taking the antibiotic, but without the antibiotic present, that phenotype may actually be detrimental, and therefore would disappear eventually.
I guess some resistance adaptations do persist, but I don't think they all necessarily do. Someone correct me if I'm wrong here.
posted by Salvor Hardin at 11:17 AM on December 13, 2010 [1 favorite]
I guess some resistance adaptations do persist, but I don't think they all necessarily do. Someone correct me if I'm wrong here.
posted by Salvor Hardin at 11:17 AM on December 13, 2010 [1 favorite]
Best answer: Is this because they are hoping that the old skool antibiotics will still nuke whatever it is you have that isn't say, antibiotic-resistant MRSA in particular?
It's not just hope-- if your infectious organism hasn't developed any antibiotic resistance, then that organism is just as vulnerable as it was fifty years ago. (Still, though, there is the aspect of hope: there's a wide variety even within a single species of bacteria, which is why you want to do a culture and sensitivity to even a known bacterium.)
So, the increasingly resistant bacterial strains are only of a particular infectious type?
Umm, no, not necessarily. There's some specific vocabulary with this stuff. "Particularly infectious" means that the organism travels from person to person particularly well. "Particularly virulent" means that the infection is particularly dangerous.
Now, antibiotic resistance isn't necessarily tied to either of these things. It's possible to evolve antibiotic resistance without affecting virulence or infectiousness. However, individual bacteria have diverse genomes, and the ones that develop resistance give their own flavor to their children. In the case of MRSA, it's not particularly infectious, but it is particularly virulent. Like all medical knowledge, this is statistically true, but not necessarily true in any particular instance. So are all MRSA developed from the same original organism? Unlikely. In a colony of MRSA, is it possible that there are some organisms that are particularly infectious but not very virulent? Possible. Is there something about particularly virulent staph that makes it prone to develop resistance? Possibly.
Shouldn't there be some antibiotics, then, that are completely useless now (or very unlikely to do jack) based on this evidence?
No. Antibiotic resistance is not that wide-spread. Resistance is the exception, not the norm.
And the resistance is, or is not, growing across the board for all types of infectious bacteria?
Gosh, that's kind of a hard one to field. Despite serious efforts in the US, my understanding is that MRSA is becoming more prevalent. We've found new resistant strains in the last ten years, and we will probably continue to do so. So yes, this is a growing problem.
But it's not growing across the board, and it's not for all types of infectious bacteria. Wikipedia's list has eight bacteria on it, and I'm not aware of any other antibiotic resistant bacteria. That's nothing compared to the number of infectious bacteria.
Vytae: ...almost any infection in the hospital is cultured before antibiotics are started.
In my experience, this isn't true. A culture and sensitivity takes days to do, and, especially among the vulnerable hospital population, infections need to be treated faster than that. If a patient has an infection, that patient will be started on broad spectrum antibiotics, informed by history and type of infection. A C&S will be run. Once the C&S is completed, the antibiotic regimen may change to one more appropriate to the specific pathogens.
posted by nathan v at 11:53 AM on December 13, 2010 [1 favorite]
It's not just hope-- if your infectious organism hasn't developed any antibiotic resistance, then that organism is just as vulnerable as it was fifty years ago. (Still, though, there is the aspect of hope: there's a wide variety even within a single species of bacteria, which is why you want to do a culture and sensitivity to even a known bacterium.)
So, the increasingly resistant bacterial strains are only of a particular infectious type?
Umm, no, not necessarily. There's some specific vocabulary with this stuff. "Particularly infectious" means that the organism travels from person to person particularly well. "Particularly virulent" means that the infection is particularly dangerous.
Now, antibiotic resistance isn't necessarily tied to either of these things. It's possible to evolve antibiotic resistance without affecting virulence or infectiousness. However, individual bacteria have diverse genomes, and the ones that develop resistance give their own flavor to their children. In the case of MRSA, it's not particularly infectious, but it is particularly virulent. Like all medical knowledge, this is statistically true, but not necessarily true in any particular instance. So are all MRSA developed from the same original organism? Unlikely. In a colony of MRSA, is it possible that there are some organisms that are particularly infectious but not very virulent? Possible. Is there something about particularly virulent staph that makes it prone to develop resistance? Possibly.
Shouldn't there be some antibiotics, then, that are completely useless now (or very unlikely to do jack) based on this evidence?
No. Antibiotic resistance is not that wide-spread. Resistance is the exception, not the norm.
And the resistance is, or is not, growing across the board for all types of infectious bacteria?
Gosh, that's kind of a hard one to field. Despite serious efforts in the US, my understanding is that MRSA is becoming more prevalent. We've found new resistant strains in the last ten years, and we will probably continue to do so. So yes, this is a growing problem.
But it's not growing across the board, and it's not for all types of infectious bacteria. Wikipedia's list has eight bacteria on it, and I'm not aware of any other antibiotic resistant bacteria. That's nothing compared to the number of infectious bacteria.
Vytae: ...almost any infection in the hospital is cultured before antibiotics are started.
In my experience, this isn't true. A culture and sensitivity takes days to do, and, especially among the vulnerable hospital population, infections need to be treated faster than that. If a patient has an infection, that patient will be started on broad spectrum antibiotics, informed by history and type of infection. A C&S will be run. Once the C&S is completed, the antibiotic regimen may change to one more appropriate to the specific pathogens.
posted by nathan v at 11:53 AM on December 13, 2010 [1 favorite]
nathan v: I agree, they start the broad spectrum antibiotics quickly. I was somewhat careless in my language, but by "before" I meant that they gather the specimen before the antibiotics are started, not that they wait around for it to grow before they start treatment. Collecting the specimen before starting the drugs is standard practice. My understanding is that this is because the drugs could affect the outcome of the tests.
posted by vytae at 12:23 PM on December 13, 2010
posted by vytae at 12:23 PM on December 13, 2010
Best answer: I walked into a clinic yesterday for a presumed sinus infection (I'm pretty darn sure it is, just knowing what they feel like for me), and after talking with the guy and him having examined my grossness, he prescribed amoxicilllin. I remember taking that as a kid, so I'd think the likelihood of it helping now is slim. No?
No. Again, the effectiveness of antibiotics and the resistance to antibiotics by bacteria is based on a huge range of strategies of bacterial metabolism. Amoxicillin, for instance, is a β-lactam based antibiotic. β-lactams function by inhibiting the synthesis of peptidoglycan in the cell wall of bacteria, causing them to lyse. Some varieties of bacteria have adapted to this by producing an enzyme called β-lactamase, which breaks the β-lactam ring and makes the chemical ineffective. One option at this point might be to throw your hands up and say, "Well, that antibiotic doesn't work anymore!" Another option is to combine the amoxicillin with a unique chemical that competitively inhibits the β-lactamase ezyme.
Thus, your doctor may still be prescribing amoxicillin, even though you have an amoxicillin-resistant bacterial infection.
What I still don't get is, shouldn't there be some antibiotics, then, that are completely useless now (or very unlikely to do jack) based on this evidence? If so, why are they still being sold?
Based on what evidence, exactly? I mean, what is the evidence saying to you; what is the evidence of?
I think the claim that you are reading from these articles (and what they are trying to suggest) is something like, "Antibiotics are working less and less, and will someday be completely ineffective altogether." That kind of a statement isn't necessarily wrong, it's just imprecise, probably intentionally-so (I mean, Newsweek...come on). The case is that by using specific antibiotics we have artificially selected for certain types of bacteria. The old types haven't disappeared completely, and we don't necessarily have ways of dealing with new types in every case. The problem as I see it isn't so much that all our antibiotics will someday become ineffective forever, but that whatever antibiotic we decide to use will always put selective pressure on the specific bacterium for resistance to that antibiotic.
There will always exist wild-type Staph aureus bacteria for which methicillin will inhibit the formation of glycan chains, it just may be seen less frequently in human infections. That does not make methicillin any less effective on non-resistant strains, it just makes non-resistant strains less common in people. It also doesn't make the non-resistant strain disappear completely, so there is always a reason to try the method that has previously proven effective. The worst that will happen is it doesn't work and you will have to try something else. Whether there can eventually exist a type of bacteria that has a resistance to every "something else" you have tried remains to be seen. Could a bacterium develop a new enzyme to lyse every inhibitor we throw at it? Could it develop a single enzyme to lyse every inhibitor we throw at it? Maybe. Is it likely? No. Does amoxicillin combined with clavulanic acid work as quickly and effectively against a resistant bacterial strain as plain amoxicillin does against a non-resistant strain? No.
I don't want to give the impression that bacterial resistance to antibiotics isn't a serious problem, because it is. Probably more because of their indiscriminate use in animals than in humans, as others have mentioned above.
Whether "resistance is, or is not, growing across the board for all types of infectious bacteria," is not even wrong. All living organisms adapt to overcome fatal threats, or else they die. The reason bacteria are here today is because their resistance to antibiotics (read: death) has been growing since the first nucleotides formed a chain.
posted by Demogorgon at 1:23 PM on December 13, 2010 [1 favorite]
No. Again, the effectiveness of antibiotics and the resistance to antibiotics by bacteria is based on a huge range of strategies of bacterial metabolism. Amoxicillin, for instance, is a β-lactam based antibiotic. β-lactams function by inhibiting the synthesis of peptidoglycan in the cell wall of bacteria, causing them to lyse. Some varieties of bacteria have adapted to this by producing an enzyme called β-lactamase, which breaks the β-lactam ring and makes the chemical ineffective. One option at this point might be to throw your hands up and say, "Well, that antibiotic doesn't work anymore!" Another option is to combine the amoxicillin with a unique chemical that competitively inhibits the β-lactamase ezyme.
Thus, your doctor may still be prescribing amoxicillin, even though you have an amoxicillin-resistant bacterial infection.
What I still don't get is, shouldn't there be some antibiotics, then, that are completely useless now (or very unlikely to do jack) based on this evidence? If so, why are they still being sold?
Based on what evidence, exactly? I mean, what is the evidence saying to you; what is the evidence of?
I think the claim that you are reading from these articles (and what they are trying to suggest) is something like, "Antibiotics are working less and less, and will someday be completely ineffective altogether." That kind of a statement isn't necessarily wrong, it's just imprecise, probably intentionally-so (I mean, Newsweek...come on). The case is that by using specific antibiotics we have artificially selected for certain types of bacteria. The old types haven't disappeared completely, and we don't necessarily have ways of dealing with new types in every case. The problem as I see it isn't so much that all our antibiotics will someday become ineffective forever, but that whatever antibiotic we decide to use will always put selective pressure on the specific bacterium for resistance to that antibiotic.
There will always exist wild-type Staph aureus bacteria for which methicillin will inhibit the formation of glycan chains, it just may be seen less frequently in human infections. That does not make methicillin any less effective on non-resistant strains, it just makes non-resistant strains less common in people. It also doesn't make the non-resistant strain disappear completely, so there is always a reason to try the method that has previously proven effective. The worst that will happen is it doesn't work and you will have to try something else. Whether there can eventually exist a type of bacteria that has a resistance to every "something else" you have tried remains to be seen. Could a bacterium develop a new enzyme to lyse every inhibitor we throw at it? Could it develop a single enzyme to lyse every inhibitor we throw at it? Maybe. Is it likely? No. Does amoxicillin combined with clavulanic acid work as quickly and effectively against a resistant bacterial strain as plain amoxicillin does against a non-resistant strain? No.
I don't want to give the impression that bacterial resistance to antibiotics isn't a serious problem, because it is. Probably more because of their indiscriminate use in animals than in humans, as others have mentioned above.
Whether "resistance is, or is not, growing across the board for all types of infectious bacteria," is not even wrong. All living organisms adapt to overcome fatal threats, or else they die. The reason bacteria are here today is because their resistance to antibiotics (read: death) has been growing since the first nucleotides formed a chain.
posted by Demogorgon at 1:23 PM on December 13, 2010 [1 favorite]
Response by poster: btw, I didn't mean to imply the Newsweek article was the basis for me asking, it was just the most recent one about bacterial resistance to antibiotics for us layfolk at the top o the google hits, so I cited it.
posted by bitterkitten at 3:19 PM on December 13, 2010
posted by bitterkitten at 3:19 PM on December 13, 2010
No worries. Reading that back I feel like it sounds a little sanctimonious, so I apologize for that. I just wish there was better information out there and less alarmist reporting.
posted by Demogorgon at 5:37 PM on December 13, 2010
posted by Demogorgon at 5:37 PM on December 13, 2010
This thread is closed to new comments.
posted by chrisamiller at 9:06 AM on December 13, 2010